What is the Nutrition Transition?
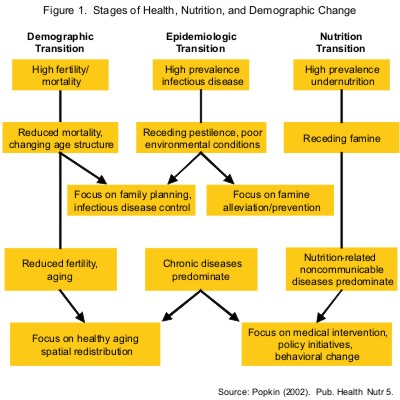
Two historic processes of change precede or occur simultaneously with the nutrition transition. One is the demographic transition: the shift from a pattern of high fertility and high mortality to one of low fertility and low mortality (typical of modern industrialized countries). Even more directly relevant is the epidemiologic transition, first described by Omran1: the shift from a pattern of prevalent infectious diseases associated with malnutrition, periodic famine, and poor environmental sanitation to a pattern of prevalent chronic and degenerative diseases associated with urban-industrial lifestyles. A third pattern of delayed degenerative diseases has been recently formulated by Olshansky and Ault2 that Accompanying this progression is a major shift in age-specific mortality patterns and a consequent increase in life expectancy. Interpretations of the demographic and epidemiologic transition share a focus with the nutrition transition on the ways in which populations move from one pattern to the next.
Large shifts have occurred in dietary and physical activity patterns. These changes are reflected in nutritional outcomes, including changes in average stature and body composition. Modern societies seem to be converging on a diet high in saturated fat, sugar, and refined foods and low in fiber, often termed the “Western diet.” Many see this dietary pattern to be associated with high levels of chronic and degenerative diseases and reduced disability-free time. These three relations are presented in Figure 1. (Download Figs 1 & 2 as PowerPoint slides)
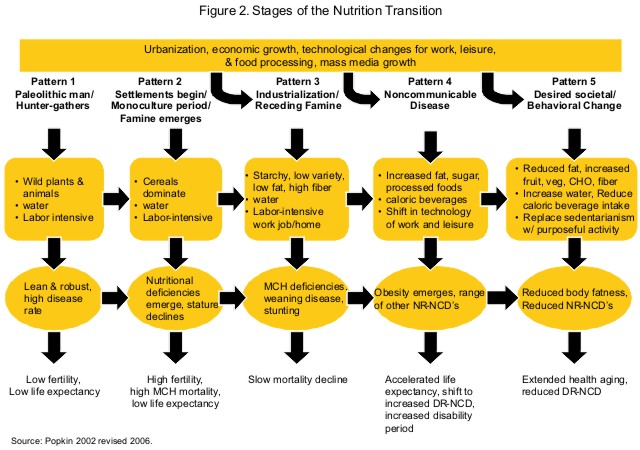
Human diet, activity patterns, and nutritional status have undergone a sequence of major shifts, defined as broad patterns of food use and their corresponding nutrition-related diseases. Over the past three centuries, the pace of dietary and activity change appears to have accelerated in varying degrees in different regions of the world. Moreover, dietary and activity changes parallel major changes in health status as well as major demographic and socioeconomic changes. Obesity emerges early in these shifts, as does the age and level of morbidity and mortality. We can think of five broad nutrition patterns. They are not restricted to particular time periods of human history. For convenience, the patterns are outlined as historical conditions/events; early patterns are not restricted to the periods in which they first arose but continue to characterize certain geographic and socioeconomic subpopulations.
Pattern 1: Collecting Food
This diet, which characterizes hunter-gatherer populations, is high in carbohydrates and fiber and low in fat, especially saturated fat.3, 4 The proportion of polyunsaturated fat in meat from wild animals is significantly higher than that from modern domesticated animals.5 Activity patterns are very high and obesity among hunter-gatherer societies is rare. Note that much of the research on hunter-gatherers is based on modern hunter-gatherers, as there is much less evidence on pre-historic people.
Pattern 2: Famine
While the variety of food becomes much less diverse, changes in diet varies across cultures and periods of acute scarcity. Dietary changes are hypothesized to be associated with nutritional stress and a reduction in stature (estimated by some at about 4 inches6, 7). During the later phases of this pattern, social stratification intensifies, and dietary variation increases according to gender and social status.8 The pattern of famine (as with each of the patterns) has varied over time and space. Some civilizations are more successful than others in alleviating famine and chronic hunger, at least for their more privileged citizens.9 The types of physical activities change but there is little change in activity levels during this period.
Pattern 3: Receding Famine
The consumption of fruits, vegetables, and animal protein increases, and starchy staples become less important in the diet. Many earlier civilizations made great progress in reducing chronic hunger and famine, but only in the last third of the last millennium have these changes become widespread, leading to marked shifts in diet. However, famines continued well into the 18th century in portions of Europe, and today they remain common in some regions of the world. Activity patterns start to shift and inactivity and leisure become part of the lives of more people.
Pattern 4: Nutrition-Related Noncommunicable Disease (NR-NCD)
In most high-income societies (and increasingly in portions of low-income societies) a diet high in total fat, cholesterol, sugar, and other refined carbohydrates and low in polyunsaturated fatty acids and fiber is often accompanied by an increasingly sedentary life. The result is an increased prevalence of obesity that leads to the degenerative diseases characterized in Omran’s final epidemiologic stage.
Pattern 5: Behavioral Change
A new dietary pattern appears to be emerging as a result of changes in diet, evidently associated with the desire to prevent or delay degenerative diseases and prolong health. These changes, which are instituted in some countries by consumers and in others by government policy, may be found to constitute a large-scale transition in dietary structure and body composition.10-12 If such a new dietary pattern takes hold, it may be very important in enhancing successful aging, i.e., postponing infirmity and increasing the disability-free life span.13, 14 Our focus is increasingly on patterns 3, 4, and 5, in particular on the rapid shift in much of the world’s low- and moderate-income countries from the stage of receding famine to NR-NCD. Figure 2 presents this focus. The concern about this period is so great that the term the nutrition transition is synonymous, for many, with the shift from Pattern 3 to 4.
References
1. Omran, Abdel R. (1971) “The epidemiologic transition: A theory of the epidemiology of population change,” Milbank Quarterly. 49: 509-38.
2. Olshansky, S.J. and Ault, A.B. (1986) “The fourth stage of the epidemiologic transition: The age of delayed degenerative diseases,” Milbank Quarterly. 64: 355-90.
3. Truswell, A.S. (1977) “Diet and nutrition of hunter-gathers,” Health and Diseases in Tribal Societies. Ciba Foundation Symposium 149, Amsterdam: Elsevier, 213-26.
4. Harris, D.R. (1981) “The prehistory of human subsistence: a speculative outline,” in D.N. Walcher and N. Kretchmer (eds.) Food, Nutrition and Evolution: Food as an Environmental Factor in the Genesis of Human Variability. New York: Masson, 1537.
5. Eaton, S.B., Shostak, M., and Konner, M. (1988) The Paleolithic Prescription: A Program of Diet and Exercise and a Design for Living. New York: Harper & Row.
6. Eaton, SB, Konner M. “Paleolithic nutrition: A consideration on its nature and current implications,” The New England Journal of Medicine. 1985; 312: 2839.
7. Vargas, L.A. (1990) “Old and new transitions and nutrition in Mexico,” in A.C. Swedlund and G.J. Armelagos (eds.) Disease in Populations in Transition, Westport, CT: Greenwood.
8. Gordon, K.D. (1987) “Evolutionary perspectives on human diet,” in F.E. Johnson (ed.) Nutritional Anthropology, New York: Liss., 341.
9. Newman, L., Kates, R.W., Matthews, R., and Millman, S. (1990) Hunger in History. Cambridge, MA: Basil Blackwell Ltd.
10. Milio N. (1990) Nutrition Policy for Food-Rich Countries: A Strategic Analysis. Baltimore: The Johns Hopkins University Press.
11. Popkin BM, Haines PS, Reidy KC. “Food consumption of U.S. women: Patterns and determinants between 1977 and 1985,” American Journal of Clinical Nutrition. 1989; 49: 130719.
12. Popkin, B.M., Haines, P.S., and Patterson, R. (1992a) “Dietary changes among older Americans, 1977-87,” American Journal of Clinical Nutrition, 55: 823-30.
13. Manton, K.G. and Soldo, B.J. (1985) “Dynamics of health changes in the oldest old: New perspectives and evidence,” Health and Society, 63: 206-85.
14. Crimmins, E.M., Saito, Y., and Ingegneri, D. (1989) “Changes in life expectancy and disability-free life expectancy in the United States,” Population and Development Review,15: 235-67.